I come from this question of gene exression analysis: Should PCA be standardized for gene expression?
My experiment is based in 151 x 51 (individuals/samples x genes), in which, patients are subjected to 3 possible groups (~ balanced groups), so we have 2 measurements of gene expression: one in the baseline, and one after the intervention. The gene expression is actually summarised in an scalar (number) called fold-change. Fold-change is calculated through the Ct (cycle threshold), which is the number of the cycle in which you are able to detect a certain amount of the target gen. This value or cycle is normalised using Ct values of 3 reference genes which are supposed to remain stable, and each patient is measured using oneself baseline value, in the same run, to remove run-to-run variation. As you can see I am working with RT-qPCR and relative quantification values.
As you can see, "normalization" or "standardization" is performed, not in the strict meaning of mathematical foundation, but to normalize quantitation of targets in the experiments. I was wondering if, taking into account that normalization is done, when I try to perform PCA to see how these genes behave, if they form cluster, if the intervention received has influence of the expression, patterns...
Reading about, I found quite divergent opinions about scaling or standardizing the results. The conflict, as far as I can see in my own experiment, lies in all my variables are genes, measured with the same high-throughput analyzer, different batches, but normalized with reference genes, and their own baseline values.
On one hand I found quite homogeneous working with scaled values, but on the other hand, I am working with values that seem to be working on the same scale, and have been through several filters to normalize results. Not sure if executing more mathematical operations could modify in the wrong way. What is your opinion about it? (all is about using the covariance matrix or correlation matrix based PCA, as far as I understand)
Furthermore, the dataset contain missing values, so I am working with the missMDA package to impute them. In case I scaled the data, what should I do first: scale or impute the missing values?
The steps to calculate fold-change:
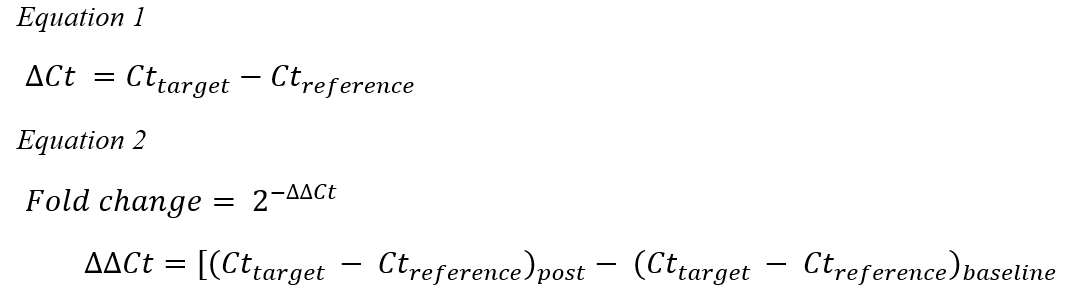
Update 1: About the technology used, is a OpenArray plate (analyzed with QuantStudio™ 12K Flex Real-Tim) which contains subarrays with customised target genes.It is a 3,072-reaction high-throughput real-time PCR. The reaction are individually performed (as far as I know, getting Ct for each sample and assay). About the 2nd point, it is 2x time series study (baseline and post-intervention)- But if you see the equations to calculate the fold-change, I am going to obtain a single value of gene expression combining the 2 Ct or measurements for each patient (as I told: baseline and post-intervention).
About the "genes aim" you can see that my interest is purely human genes, after an intervention (inflammation-related genes).
About the pippeting issue. As you know is never discarded, but the internal controls or reference genes (as I am adressing them) goal is to normalize results and remove potential quantification errors. However, as you said the RNA concentration (A260) and purity were calculated spectrophotometrically from peripheral blood samples origin
As far as I know, the terms correlation and covariance related to PCA, are meant to discrimanate the standardization process (in correlation matrix) and not standardized matrix (scale function in R). Not sure if I understood this is what you imply?
My guess is nowadays everything is RNAseq and microarrays, whose mechanisms, and therefore, statistical preprocesses are different from RT-qPCR. But there are papers of PCA working wiht data coming from RT-qPCR. Shouldn't it work though?
Update2
Covariance and correlation: "Covariance analysis of PCA: PCA is dimensionality reduction based on maximising multi-dimensional variance so that would be unusual, but correlation matrix of PCA is understandable. Normally covariance analysis is performed directly on standardised data." Let me insist on this topic a little bit more.I am not sure if I understood correctly what you stated, but the information I've reviewed seems to say otherwise. As far as I was able to find, https://aedin.github.io/PCAworkshop/articles/b_PCA.html : "PCA was computed as a singular value decomposition (SVD) of a column centered, scaled matrix. This was PCA of the correlation matrix. If the matrix is centered but not scaled, it is PCA of the covariance matrix." I am not sure if I understood correctly what you stated, but the information I've reviewed seems to say otherwise
"The correlation matrix is the standardized version of the covariance matrix. Analysing the correlation matrix is a useful default method because it takes the standardized form of the matrix; therefore, if variables have been measured using different scales this will not affect the analysis. Often you will want to analyse variables that use different measurement scales. Analysing the correlation matrix ensures that differences in measurement scales are accounted for. In addition, even variables measured using the same scale can have very different variances and this too creates problems for principal component analysis. Using the correlation matrix eliminates this problem also. There are statistical reasons for preferring to analyse the covariance matrix (the reason being that correlation coefficients are insensitive to variations in the dispersion of data whereas covariance is and so produces better-defined factor structures (Tinsley & Tinsley, 1987)) and generally the results will differ from analysis on the correlation matrix. However, the covariance matrix should be analysed only when your variables are commensurable." Conclusion: shouldn't it be the covariance matrix the one without standardized values, because variables share same scale?
Missing values: this is an issue, at least with several functions in R (prcomp(), princomp())which don't work with NAs in the matrix.
About this statement: "The key question, which is standardisation and I would say it is essential for RT-qPCR derived data at a minimum to at least investigate consistency of signal against a control. That minimum is what the second equation describes (why it works is complicated)."
I don't really understand what you mean standardize at a minimum. The endogenous control genes we are using are individualized for every sample. Let say we are investigating the fold-change in the individual i and the variable k. We are using endogenous controls in the i individual to "standardize" values. The